
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()

click on image to view video
Written and produced by Dr. Sue Pavord,
Consultant Haematologist and
Lecturer at University of Leicester Medical
School
A bone marrow aspiration or biopsy is usually done by a hematologist, medical oncologist, internist, or pathologist, or by a trained technologist. This biopsy may be done in doctor's office or in a hospital.
Adults usually have a sample of bone marrow fluid taken from the back of the pelvic bone. In rare cases, a fluid sample is removed from the sternum or from the front of the pelvic bone. Babies and young children may have the sample taken from the front of the lower leg bone, just below the knee.

|
The patient is placed in the lateral decubitus position, with the top leg flexed and the lower leg straight |

Obtained from: http://emedicine.medscape.com/article/207575-overview
| Palpate the iliac crest, and mark the preferred sampling site with a pen. | |
| Aseptic technique must be used (sterile gloves and gown etc) | |
| The site is prepared with an antiseptic, scrubbed, and draped, exposing
only the site to be sampled.
|
| The skin and the underlying tissue to the periosteum are infiltrated with a local anesthetic. A 10-mL syringe with a 25-gauge needle is used to inject an initial 0.5 mL directly under the skin. A 22-gauge needle is used to penetrate deeper into the subcutaneous tissue and the underlying periosteum. |
| Adequacy of the anesthesia is tested by gently prodding the periosteum with the tip of the needle and asking the patient for any painful sensation. |
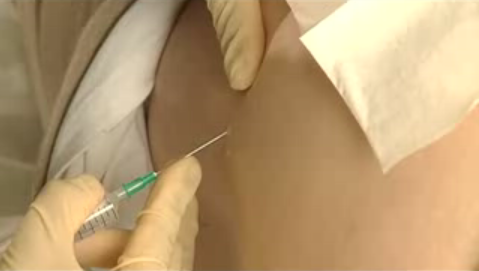
| A skin incision is made with a small surgical blade, through which the bone marrow aspiration needle, with a stylet locked in place, is inserted. |
| Once the needle touches the bone, it is advanced slowly until the cortical bone is penetrated and the marrow cavity is entered. Contact with the marrow cavity is usually noted by a sudden reduction in pressure. The depth of the penetration should not extend beyond an 1 cm. |
| Once within the marrow cavity, the stylet is removed. Using a 20 mL syringe, approximately 0.3 mL of bone marrow is aspirated. A volume greater than 0.3 mL may dilute the sample with peripheral blood and thus is not recommended. The material collected for bone marrow slides is generally not mixed with an anticoagulant, this avoids any cellular morphologic artifacts. If there is to be a delay in slide preparation, place the sample in an EDTA anticoagulant-containing tube. |
| If additional marrow is needed, subsequent specimens are obtained by attaching a separate syringe, collecting 5 mL at a time. The samples are then transferred into an anticoagulant-containing tube that is appropriate to the requested study: heparin for cytogenetic analysis; either heparin or EDTA for immunophenotyping; formalin for a Cytoblock preparation; and, gluaraldehyde for ultrastructural examination. |

Obtained from: http://emedicine.medscape.com/article/207575-overview
|
The marrow needle is removed, and pressure is applied to the aspiration site with gauze until bleeding has stopped. |
![]()
Your comments and enquiries are most welcomed!
Ó
Copyrights Reserved
![]()
